
Ask the Expert: An Interview with Nate Lawson, DMD, PhD on Dual-Cure Bulk Fill Composite
By Nate Lawson, DMD, PhD
Question
How does the dual-cure mechanism work in comparison to light-cure?
Answer
Dual-cure composites have chemical cure initiators in them that allow polymerization of the resins when the two components of the chemical cure initiators come into contact. Dual-cure materials will always be supplied in dual-barrel syringes in order to separate the components of the chemical cure initiators.
Question
How long does it take for a dual-cure bulk fill composite to fully self-cure? Is there any difference in the working time of a dual-cure bulk fill and a light-cure composite, and does depth of cure affect that time?
Answer
The working time of a dual-cure composite will be shorter than a light-cured composite. The working time will be material dependent. The speed of the chemical curing component will be balanced by prolonging the working time of the material while expediting the chemical cure of the material.
I can’t think of a reason why working time would affect depth of cure (or maximum depth of a restoration). I don’t see a disadvantage if the material on the floor of the restoration begins to harden while the operator is still dispensing material into the occlusal aspects of the tooth. In fact, polymerization initiated on the floor of the preparation before the occlusal aspect of the preparation is a strategy to prevent polymerization forces from debonding the restoration from the floor of the preparation.
Question
What are the handling properties of a dual-cure bulk fill composite?
Answer
Dual-cure materials are dispensed from dual-barrel syringes. The handling properties of the material should be viscous enough to prevent excessive flow when handling but not too viscous to prevent easy dispensing from the dual-barrel syringe. Just as there is a range of viscosities of light-cure materials, there is also a range of viscosities of dual-cure materials. Some dual-cure materials require dispensing guns due to the viscosity of the composite. Most dual-cure composites handle similarly to a flowable composite.
Question
What is the recommended placement technique for a bulk fill composite?
Answer
The recommended placement technique for a bulk fill composite is to start in the deepest part of the cavity to ensure that the composite material fully contacts the base of the preparation, reducing the risk of air entrapment or voids. Continue to fill the preparation ensuring the placement tip remains submerged within the composite throughout completion of the cavity filling. To avoid excess flow due to gravity (i.e., restoring an upper molar), the initial increment of bulk fill material may be light-cured for 5 seconds followed by immediate placement of more bulk fill composite.
Question
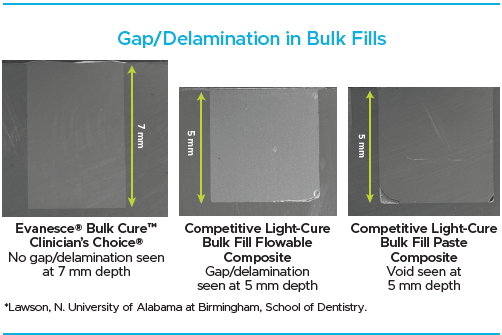
What are the benefits of dispensing one increment of composite in a deep restoration versus layering materials? Are there known issues with gaps and/or bubbles in between layers?
Answer
Although gaps between layers of composite are probably not as detrimental to a restoration as gaps between the first layer of composite and the tooth, placement of composite in layers does allow the introduction of gaps and voids. The gaps can be places for stain or plaque accumulation.
Question
What adjustments are needed to the adhesive protocol when using a dual-cure composite, and how does the dual-cure material interact with the dental bonding agent compared to a light-cure composite?
Answer
It is imperative to use a compatible adhesive with a dual-cure composite. If a self-etch single bottle adhesive or universal adhesive is used before using a dual-cure composite, the acidity of the adhesive can prevent the chemical cure of the dual-cure material. Therefore, it is necessary to either:
- Use an adhesive that is not acidic (2-bottle adhesive or total-etch adhesive)
- Use a dual-cure material that is amine-free
- Use a dual-cure activator with the single bottle self-etch adhesive
Question
What are the differences in shrinkage rates and polymerization stresses between dual-cure and light-cure systems? How does dual-cure system handle stress management in deep cavities?
Answer
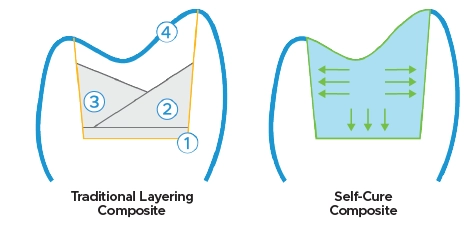
Dual-cure materials undergo slower chemical polymerization before light activation, allowing for delayed gelation and stress relaxation, which reduces shrinkage stress (Hughes Oper Dent 2019). This minimizes issues like marginal failure, postoperative sensitivity, microleakage, secondary caries, and tooth fracture, which are common with light-cured composites.
With light-cure systems, increment thickness and curing time/intensity essentially maximize shrinkage forces and stress development which increases the chance of post-operative sensitivity and other clinical failures.
Question
How does the use of a dual-cure bulk fill composite affect the overall efficiency of a procedure or chair time?
Answer
The advantage of dual-cure materials in terms of efficiency is that the restoration placement is faster than that of layering composites. There are two reasons for this. First, the consistency of the material allows good adaptation, similar to a flowable composite, and the properties (esthetic and mechanical) will enable the material to be filled to the occlusal surface. Therefore, this material has the advantage of being both a flowable and packable composite without switching materials. Second, this material’s unlimited depth of cure allows the entire preparation to be filled in one increment without stopping to perform light-curing or reinserting the composite syringe.

ABOUT THE AUTHOR
Dr. Lawson is the Director of the Division of Biomaterials at the University of Alabama at Birmingham School of Dentistry and the program director of the Biomaterials residency program. He graduated from UAB School of Dentistry in 2011 and obtained his PhD in Biomedical Engineering in 2012. His research interests are the mechanical, optical, and biologic properties of dental materials and clinical evaluation of new dental materials. He was the 2016 recipient of the Stanford New Investigator Award and the 2017 3M Innovative Research Fellowship both from the American Dental Association. He served on the American Dental Association Council of Scientific Affairs and is on the editorial board of The Journal of Adhesive Dentistry and Compendium. He has lectured nationally and internationally on the subject of dental materials. He also works as a general dentist in the UAB Faculty Practice.
Share This Article! Choose Your Platform
Products Mentioned in this article
Related Articles

Ask the Expert: An Interview with Nate Lawson, DMD, PhD on Universal Adhesives
By Nate Lawson, DMD, PhD
What is an universal adhesive? A “universal” adhesive is not a technical term but rather a clinical term. It implies that an adhesive can be used with or without phosphoric acid on dentin or enamel. In scientific writing, these adhesives are sometimes referred to as mild self-etch adhesives because they have a slightly less acidic pH (around 3) than typical self-etch materials (around 2).

Ask the Expert: An Interview with Matthew R. Miller, DDS on Sectional Matrix Systems
By Matthew R. Miller, DDS
There are many sectional matrix systems on the market today. Are some better than others? What should I be looking for when choosing a sectional matrix system?

Ask the Expert: An Interview with Ed Lowe, DMD, AAACD on Soft Tissue Diode Lasers
By Ed Lowe, DMD, AAACD
What type of clinical procedures can be done with a soft tissue diode laser?